



Introduction
Various factors, including advancements in treatment methods, early detection screenings, and improved surgical techniques, have contributed to a notable increase in breast cancer survival rates. In the United States, the 5-year survival rate for breast cancer patients was 91% in 2018 [1]. Meanwhile, in South Korea, the rate rose from 77.9% between 1993 and 1995 to 93.8% between 2016 and 2020 [2]. With these trends, breast cancer survivors may live for many decades. Therefore, it is crucial to develop strategies aimed at enhancing their quality of life while effectively managing the risks of recurrence and mortality.
Breast cancer treatment can lead to psychological and emotional side effects. These not only negatively affect the patientŌĆÖs quality of life but also result in increased economic burdens, such as productivity losses. As such, it is crucial to provide ongoing interventions and management to support breast cancer patients during and after their treatment [3]. Encouraging self-care and implementing programs that promote healthy lifestyle habits can enhance health outcomes, boost self-efficacy, and lower the risks of cancer recurrence and mortality [4]. Exercise and diet play a significant role in maintaining a healthy lifestyle, which is essential for the well-being of breast cancer patients. Therefore, interventions designed to improve lifestyle habits, including various exercise routines and dietary changes, have been introduced [5,6]. However, these interventions tend to have only short-term effects, highlighting the need to devise strategies that extend their benefits [7,8].
Since the onset of the coronavirus disease 2019 pandemic, eHealth platforms such as websites and video conferencing have seen rapid expansion [9,10]. Telemedicine has provided scalable and flexible methods for healthcare support, effectively replacing many in-person appointments and ensuring continuity of care [11]. Technology-based interventions involve the use and implementation of technological tools or methodologies in the design, development, and distribution of healthcare solutions to target participants [12]. These interventions also utilize readily accessible devices like smartphones, the internet, or mobile sensors to monitor, reinforce, or provide convenient and cost-effective healthcare services to individuals in need of medical care [12]. Notably, technology-based interventions have demonstrated high patient preference in terms of acceptability and utility, fostering patient-centered care through standardization [13]. They also allow breast cancer survivors to share their experiences and provide immediate feedback to healthcare professionals, facilitating real-time interaction [14]. Therefore, technology-based interventions offer patients a convenient and engaging way to continuously receive health assessments, education, symptom management, self-management enhancement, and psychosocial support [15,16].
Moreover, various technologies, such as online chat platforms, diary writing, video-based education, video games, websites, social media platforms, and mobile applications, have been utilized to promote health and provide psychosocial support for breast cancer survivors [17,18]. Given the intensive and long-term treatment required by breast cancer patients, along with their self-management needs, the provision of timely care is crucial for improving overall self-management in this group [19,20]. Consequently, these technology-based self-management interventions allow breast cancer survivors to access timely and effective treatments. They offer a broad array of resources and tools that can improve their health outcomes and foster their psychosocial well-being [21-23].
The effects of mobile health interventions on physical activity and patient-reported health outcomes, such as quality of life, stress, fatigue, and sleep, in patients with breast cancer have been increasingly examined through systematic reviews [24,25]. However, many of these studies have concentrated on a single type of technology or health outcome, making it challenging to assess the interventionŌĆÖs acceptability among the target population and the overall trends in which variables self-management programs have been applied and their effectiveness. Consequently, a study that includes various technology-based interventions, such as mobile health, eHealth, and artificial intelligence (AI), and evaluates functionality acceptance, utility, engagement, and long-term management should be undertaken. This would provide the necessary information for developing innovative technology-based interventions and minimizing unnecessary costs [26]. The variety in intervention approaches and outcome assessments in technology-based self-management interventions for breast cancer complicates comparisons, and systematic literature reviews that include interventions using multiple media are scarce. Therefore, this systematic review was conducted with the aim of improving our understanding of technology-based self-management interventions and assessing various health outcomes during and after treatment, thereby providing directions for future research. The findings of this study will contribute to the foundational knowledge of intervention development by understanding the characteristics and outcomes of technology-based self-management interventions for women with breast cancer. The review questions were:
1. What do technology-based self-management programs consist of, and what do they provide to women with breast cancer?
2. What outcomes have been evaluated among women with breast cancer after self-management programs?
3. What is the structure of technology-based self-management programs?
METHODS
Study design
This systematic literature review, which focused on technology-based self-management programs for women with breast cancer, adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [27].
Eligibility criteria
To clarify the inclusion criteria and devise an effective search strategy, we utilized the PICO (Population/Intervention/Control/Outcome) framework [28]. The population for this study comprised women diagnosed with breast cancer, specifically those undergoing treatment and survivors who had completed treatment. The intervention involved a technology-based approach incorporating elements of self-management. This systematic review did not employ a comparison group. While the outcome was not restricted, it was necessary to measure one or more quantitative outcomes to assess the effectiveness of the self-management interventions. We included studies written in either English or Korean that were published in peer-reviewed academic journals.
In this context, technology-based interventions refer to the application of information communication technologies in facilitating the delivery of education and care for health-related conditions [28]. These interventions can be broadly categorized into two types: internet-based and mobile-based [29]. Therefore, in this study, technology-based interventions encompass all internet- and mobile-based technologies utilized in providing health-related information and care to women diagnosed with breast cancer.
Studies were excluded if they: (1) were review papers, editorials, case studies, or protocols, (2) did not specifically address womenŌĆÖs health in relation to breast cancer, and (3) failed to provide detailed information about the intervention.
Our primary outcome of interest was symptoms directly associated with the disease. Secondary outcomes included aspects of psychological health such as quality of life, depression, and anxiety, among others. Physical health factors, including fatigue, diet, and physical activity, were also of interest. Additionally, we considered other health-related outcomes, such as medication compliance.
Search strategy
From May 23 to June 12, 2023, two researchers comprehensively retrieved studies in five English databases and two Korean databases. These databases included PubMed, the Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Web of Science, Cochrane Central Register of Controlled Trials, Research Information Sharing Service, and Data Base Periodical Information Academic (Appendix 1). The researchers used the following keywords for each database: (breast cancer) AND (mobile OR m-health OR e-health OR web OR app* OR technology-based OR artificial intelligence OR AI OR chatbot OR telehealth OR digital health) AND (self-management OR self-help OR self-care OR self-guided OR self-administ*) AND (program OR intervention). There were no restrictions on the publication date, and search sets were combined using Boolean operators. Additionally, the researchers conducted backward and forward searches of the identified publications to locate other relevant materials.
Study selection and data extraction
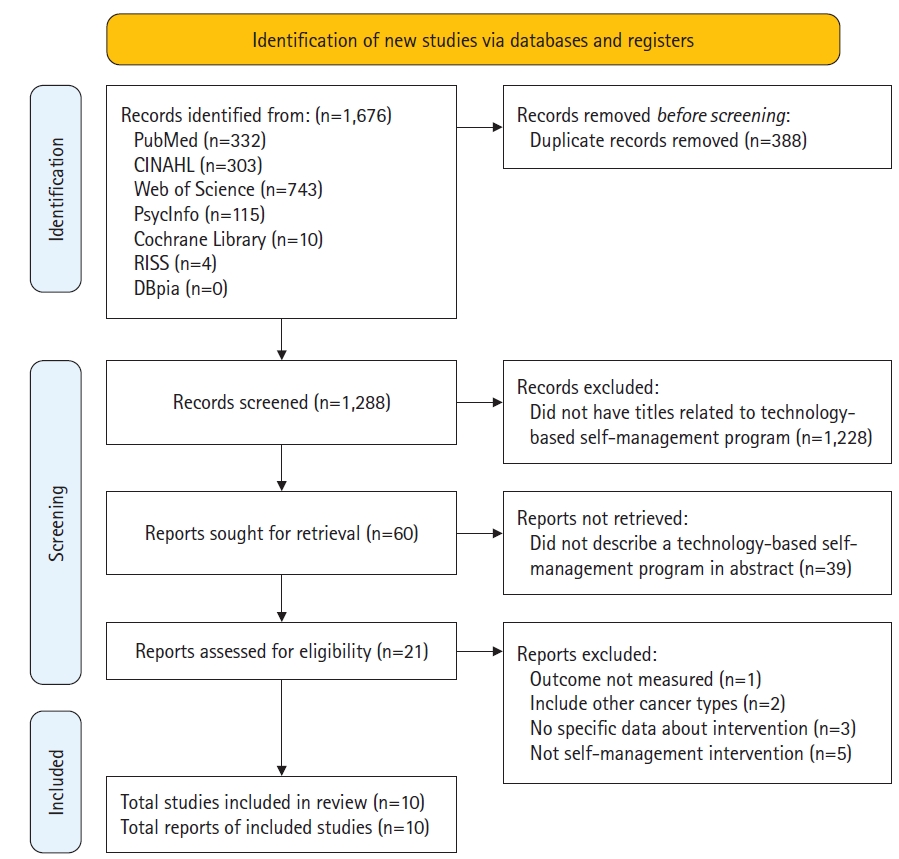
Studies were selected in accordance with the PRISMA guidelines. Following the pooling of literature search results, any duplicates were eliminated. Two independent reviewers assessed the titles and abstracts based on the inclusion and exclusion criteria of the studies. Subsequently, the full text of potentially relevant studies was reviewed by two individuals, who then made the selection. Any disagreements between the reviewers were resolved through discussion. The number of studies excluded, along with the reasons for their exclusion, were recorded in a PRISMA flowchart, as depicted in Figure 1.
Using a Microsoft Excel template, two reviewers extracted data from each of the listed studies. The detailed information included the first author, publication year and country, study design, sample/population, sample size, main intervention, control group, study outcome, main findings, and intervention characteristics (technology, program contents, duration, session, intervention manager, intervention manager involvement, and follow-up). The extracted data were subsequently cross-verified to ensure the accuracy of the data extraction process.
Assessment of risk of bias
Two independent reviewers assessed the quality of the studies included in this review. Any disagreements that arose were resolved through discussion. Specifically, the quality of randomized controlled trials (RCTs) was evaluated using the Cochrane Risk of Bias 2.0 (RoB 2.0) tool. For nonrandomized interventional studies, the Risk of Bias in Nonrandomized Studies-of Interventions (ROBINS-I) tool was employed. The RoB 2.0 toolŌĆÖs evaluation algorithm was used for each domain to determine whether there was a ŌĆ£low risk,ŌĆØ ŌĆ£some concerns,ŌĆØ or ŌĆ£high riskŌĆØ of bias. The ROBINS-I tool identified five categories of bias risk across seven domains: ŌĆ£low risk of bias,ŌĆØ ŌĆ£moderate risk of bias,ŌĆØ ŌĆ£high risk of bias,ŌĆØ ŌĆ£very high risk of bias,ŌĆØ and ŌĆ£no information.ŌĆØ
RESULTS
Characteristics of selected studies
Out of 1,288 studies identified through an electronic database search, 10 (Appendix 2) were included in this review following a full-text screening, which were named from A1 to A10 [30-39]. Studies with unmeasured outcomes or those that did not focus on self-management interventions were excluded (Figure 1). Three of the studies (A2, A5, and A8) were conducted in the United States, two (A1 and A10) in Europe (specifically the Netherlands and Norway), three (A3, A4, and A7) in East Asia (South Korea), and two (A6 and A9) in the Middle East (Egypt and Iran). Seven of the included studies were RCTs, two were nonrandomized interventional (i.e., quasi-experimental) studies (A6 and A7), and one was a cross-sectional study (A5). The sample sizes ranged from 24 to 355. The control intervention was primarily usual care (80%), with two studies providing an educational booklet (A3 and A4). In the majority of the studies (70%), the follow-up period was identical to the program duration, and the post-test was conducted immediately after the programŌĆÖs conclusion (A2, A3, A4, A5, A6, A8, and A9). Three studies followed up on program outcomes at 2, 3, and 6 months after the program ended (A1, A7, and A10).
Risk of bias
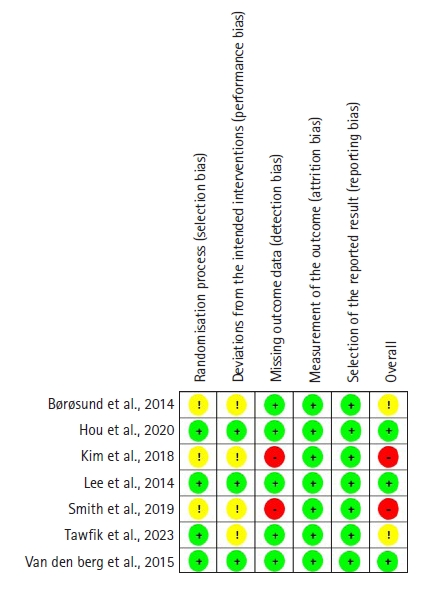
Figure 2 shows the methodological quality of the RCTs. Using the RoB 2.0 tool, we conducted a Cochrane risk of bias analysis on the RCTs. Three of the seven RCTs did not report allocation concealment (A1, A3, and A8), which raised potential concerns regarding selection bias. Given the inherent characteristics of psychosocial interventions, it is challenging to blind participants, which inevitably resulted in performance bias in four studies (A1, A3, A8, and A9). Two studies failed to detail their approach to handling missing data (A3 and A8), thereby elevating the risk of detection bias. However, no significant attrition bias or reporting bias was observed.
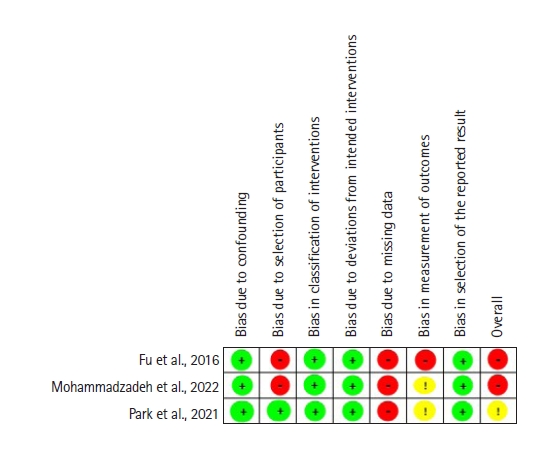
Figure 3 depicts the methodological quality of non-RCTs. Using the ROBINS-1 tool, we conducted a Cochrane risk of bias analysis on the non-RCTs. All three non-RCTs demonstrated a high risk of detection bias due to the absence of a description of how dropouts and missing data were handled (A5, A6, and A7). Furthermore, the absence of a control group or a well-defined description of the control group presented a high risk for the classification of the intervention (A5 and A6).
Technology
The interventions could be broadly categorized into two primary types: those that relied on internet platforms and those that depended on mobile platforms. Of the 10 articles included in our final sample (Table 1), five utilized mobile-based interventions (A2, A3, A5, A6, and A7), four employed web-based interventions (A1, A4, A8, and A10), and one used a web-based intervention that incorporated a chatbot (A9). A common theme across these studies was the assertion that technology-based interventions, such as web-based and mobile-based programs, can provide patient-centered care. This allows patients to evaluate their symptoms at any time and from any location. A unique feature of the mobile-based programs was the inclusion of an innovative training system that used avatar simulation videos to help breast cancer survivors develop self-care skills (A5). Additionally, the web-based program that utilized an AI chatbot offered personalized education tailored to womenŌĆÖs needs. This allowed women to engage in individual conversations and receive customized information based on their specific questions (A9).
Programs
Constructs
The results identified several common constructs in the self-management programs (Table 2). The most commonly observed constructs were those related to the provision of information and communication to assist patients in effectively managing their condition (A1 and A2). Constructs associated with assessment, as well as planning with a diary to improve patientsŌĆÖ knowledge, encourage proactive actions, and efficiently monitor their progress, were also prevalent (A1, A3, A4, and A7). Numerous programs focused on specific symptom management and self-care strategies, aiming to equip patients with the necessary skills and knowledge to manage their symptoms and overall health effectively (A5, A6, and A7). Additionally, a handful of programs incorporated cognitive-behavioral therapy and cognitive reframing to offer personalized support, foster active participation, and enhance patientsŌĆÖ comprehension and coping abilities (A8 and A10).
Manager involvement
Five of the 10 studies incorporated the involvement of intervention managers during the interventions (A1, A3, A6, A7, and A8). The strategies varied among the studies. In one study, users were given access to a ŌĆ£Contact UsŌĆØ section within the app, which allowed them to pose questions at any time (A6). Another study conducted weekly interviews with participants via cell phone throughout the duration of the study. This consistent communication enabled healthcare personnel to continuously monitor and support the patients, providing a uniform and personalized intervention experience (A3). A different strategy involved offering a platform for patients to seek assistance from healthcare personnel at their treatment hospital. This platform enabled patients to ask questions, share experiences, and receive advice from oncology nurses. If necessary, the nurses could also direct further inquiries to physicians and social workers, ensuring comprehensive support and expertise (A1). In another study, participants received regular weekly feedback via email, which encouraged them to consistently engage with the website, learn about self-management, and maintain their health diary. This continuous communication and feedback loop was designed to foster active participation and adherence to the intervention among patients (A7). In a separate study, an online group meeting was facilitated by masters who were equipped with a prepared and certified Pillar Guide (A8).
Health-related outcomes
Table 3 lists the health-related outcome variables in the 10 self-management programs. For women with breast cancer, these 10 articles discussed 12 health-related outcome variables. With respect to the primary outcome, the program exhibited positive effects in diminishing pain symptoms (A5, A6, and A8) and mitigating distress and side effects (A1, A3, A5, A9, and A10). It also effectively managed menopausal symptoms (A7). Regarding psychological health, a secondary outcome, the program yielded encouraging results in reducing anxiety (A1 and A4), depression (A1, A4, and A8), fear of cancer recurrence (A10), and in improving quality of life (A2, A3, A5, A6, and A7), self-efficacy (A4, A8, and A10), and empowerment (A10). In terms of physical health, the program was beneficial in alleviating fatigue (A4, A6, A8, and A10) and enhancing dietary quality (A4). Additionally, the program showed positive outcomes in relation to medication compliance (A3).
DISCUSSION
This systematic review examined technology-based self-management programs designed for supportive care in women with breast cancer, focusing on their content and outcomes. Generally, the methods employed in these self-management programs are somewhat limited, and there is a broad range of variation in both content and outcome variables across different studies. Nevertheless, this review can offer guidance on the factors that should be considered when developing and implementing more effective technology-based self-management programs for women with breast cancer.
Web-based technology currently dominates the field of self-management programs for women with breast cancer, with mobile technology, utilizing devices such as smartphones and tablets, coming in second. Web-based intervention programs have long been favored for their ability to provide timely information and support when necessary [40,41]. Concurrently, the use of mobile technology in self-management interventions for individuals with chronic diseases is on the rise, due to its accessibility and portability. This technology enables patients to self-monitor their symptoms at any time and place [36,42].
Five of the 10 studies included in this review focused on mobile-based interventions. Of these, four studies employed applications, with the exception of the study of Fu et al. [34], which incorporated avatar simulation videos. Mobile applications are viewed as highly suitable and effective tools for self-management. They offer the ability to monitor not only specific symptoms, but also physiological indicators and daily activities such as diet and exercise [43]. Consequently, mobile applications can be effectively used not only for tracking post-treatment symptoms in women with breast cancer, but also for promoting health. It is suggested that further studies be conducted to monitor daily activities like diet and exercise among women with breast cancer using mobile applications. This could serve as a method for promoting the health of women with breast cancer.
In the study of Tawfik et al. [38], which is the most recently published study among those included, an AI chatbot was used for a self-management intervention. The study found that ChemoFreebot, an AI technology, significantly impacted womenŌĆÖs self-care behaviors and mitigated chemotherapy-related side effects [38]. AI chatbots are acknowledged as effective self-management tools, as they can minimize the need for face-to-face consultations and offer further evaluation and self-management advice based on the patientŌĆÖs response [44]. Considering research that suggests cancer patients require more personalized and tailored information [45], AI chatbots could be a valuable tool for enhancing self-management. While there is still some technical work to be done, AI chatbots hold promise as a healthcare tool and signify a substantial technological advancement [44]. Currently, this self-management program primarily employs web and mobile technologies, but it is progressing by integrating newly developed technologies. Therefore, it is recommended to further develop a self-management program using AI to demonstrate its effectiveness. Moreover, the effectiveness of AI-based interventions should be compared with web/mobile-based self-management programs to determine which technologies can most effectively deliver self-management programs.
The outcomes assessed by self-management programs for women with breast cancer can be categorized into physical symptoms and psychological factors associated with the disease. Physical symptoms, such as menopausal symptoms, fatigue, and pain, showed considerable variation across the studies included. Among the psychological factors, quality of life was the most frequently measured. However, the instruments used to gauge quality of life varied significantly across the studies [31,34,35], complicating the comparison of results. Despite this, the implementation of self-management programs has consistently demonstrated an improvement in quality of life. To strengthen the evidence of a programŌĆÖs effectiveness, future studies could employ the same instrument to evaluate quality of life or examine the sustainability of the effectiveness. Following quality of life, self-efficacy was the second most frequently measured factor. According to the transtheoretical model, self-efficacy is a determinant that can instigate behavioral change and ultimately enhance quality of life [46]. This factor also serves as a crucial psychosocial resource for self-management programs to be effective for participants [37]. Therefore, self-efficacy is not only a factor that can be positively influenced by self-management programs, but it is also a key determinant for participants to maintain self-management and carry out positive changes.
Regarding the constructs of self-management programs, we found that despite variations in specific program structure and content across different studies, several elements were consistently present. These elements encompassed the provision of information via educational materials, symptom self-management, plan creation, and the provision of psychological support through communication. The integration of these constructs into self-management programs is intended to empower patients, enhance their knowledge and skills, improve symptom management, and foster overall well-being. It is noteworthy that the use of a health diary as a self-management tool effectively bolstered self-efficacy in self-management [30,33,36]. This health diary incorporated self-management strategies, goal-setting activities, and a self-report form [36]. Participants were encouraged to evaluate their daily execution of health-enhancing behaviors and record the extent of their implementation as part of their self-management process [30,33]. This, in turn, motivated them to refine their behaviors and adopt healthier lifestyle patterns [33]. The use of a health diary played a significant role in enhancing self-efficacy in self-management. Its purpose aligns with the objectives of self-management programs, which are to motivate patients to self-manage by enhancing their disease understanding, and to enable them to monitor their health changes and respond appropriately. Given that programs incorporating these elements effectively reduce symptoms and improve self-management, it may be beneficial to consider these elements when designing self-management programs.
Another interesting finding of this review is that the programsŌĆÖ structure incorporated a communication component, which enabled patients to share their experiences. In one study, patients had the opportunity to participate in online forum discussions, allowing them to anonymously exchange messages with other patients or use a blog platform. This feature provided patients with the reassurance that someone was available to address their concerns, thereby offering psychological support [34]. In a similar vein, another study included a community section where patients could share their thoughts and experiences [36], and senior survivors and healthcare professionals could distribute uplifting information [31]. Social support plays a pivotal role in the life of a cancer patient, potentially transforming their lives by bolstering their will to live [47]. Therefore, patient-to-patient communication within the self-management program could be a key factor in enhancing the programŌĆÖs effectiveness.
In some studies, intervention managers utilized a variety of strategies, such as being continuously available, conducting regular interviews, and providing consistent feedback throughout their involvement in the program. However, many of the studies included did not involve the intervention manager at any stage in the program, instead allowing participants to navigate the program independently. The results indicated a significant positive impact on outcomes immediately following the intervention program [31,35]. Shi et al. [48] conducted a systematic review of mobile-based self-management programs for symptoms related to chemotherapy in breast cancer patients undergoing treatment and found that a self-management program without an intervention manager had a significantly positive effect. This aligns with our findings, suggesting that a well-structured self-management program can be effective for participants without the need for advice or feedback from an intervention manager. However, Harrington [49] argued that the ŌĆ£involvement of the intervention managerŌĆØ is a crucial factor in enhancing participantsŌĆÖ health-related outcomes in self-management programs. Support from healthcare providers is reported to be particularly necessary for application-based interventions. Therefore, further research is required to determine whether the effectiveness of the self-management program varies depending on the need for an intervention manager.
This study has several limitations. First, the outcomes varied across the studies, and the tools used were different. Therefore, caution should be taken in interpreting the results. Second, this review only included studies using quantitative measures; thus, important insights from qualitative research may have been missed. Third, many studies did not describe attrition rates or refusals, raising questions about selection bias.
This systematic review offers insights into the structure, measured outcomes, and effectiveness of technology-based self-management programs for women with breast cancer. The most commonly utilized technologies in these programs are web- and mobile-based; however, there has been a recent trend towards incorporating new technologies. No consistent trends in study outcomes were observed due to the significant variation across studies. Despite this, we identified several promising findings within individual studies, particularly the significance of self-efficacy and key components of self-management programs. ItŌĆÖs also important to consider certain factors when designing a self-management program for women with breast cancer, such as the crucial role of communication and the potential inclusion of an intervention manager. Future research should continue to evaluate and confirm the effectiveness of technology-based self-management programs for women with breast cancer, with the aim of helping these women overcome their physical and psychological challenges and enhance their quality of life.